65 yr old female cva case
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
Patient and his/her attenders have been informed and their consent has been taken.
A 65 yr old female was brought to the casualty with complaints of
• Difficulty in moving upper limbs and lower limbs since 3 days
• Unable to speak since 3 days
𝐇𝐈𝐒𝐓𝐎𝐑𝐘 𝐎𝐅 𝐏𝐑𝐄𝐒𝐄𝐍𝐓𝐈𝐍𝐆 𝐈𝐋𝐋𝐍𝐄𝐒𝐒:
Patient was apparantly assymptomatic 3 days back, then she developed weakness in left upper and lower limbs ( on Saturday afternoon )which was sudden in onset , gradually progressed first appeared in the upper limb and then in the lower limb associated with slurred speech and was trying to convey something. On Sunday afternoon weakness developed into left sided hemiplegia developed and complete loss of speech occured
• No H/O Head Trauma (for haemorrhagic stroke)
• No H/O Epilepsy
• No H/O projectile vomiting, headache or blurring of vision
• No H/O recent surgeries (for embolic stroke)
𝐏𝐀𝐒𝐓 𝐇𝐈𝐒𝐓𝐎𝐑𝐘 :-
• No H/O similar complaints in the past
• She is a hypertensive and is on medication since 2 years
• No H/O DM, TB, Hypo/Hyperthyroidism/ Epilepsy/ Asthma/COPD/ CAD/ Blood transfusions/ Connective tissue disorders (stroke in young)
• No H/O Major hospitalizations
• No H/O major surgeries
𝐏𝐄𝐑𝐒𝐎𝐍𝐀𝐋 𝐇𝐈𝐒𝐓𝐎𝐑𝐘 :-
• Patient is married
• Occupation: Homemaker
• Diet : Mixed diet
• Appetite : decreased
• Bowel & bladder movements are normal
• No known allergies
• No addictions
𝐆𝐄𝐍𝐄𝐑𝐀𝐋 𝐄𝐗𝐀𝐌𝐈𝐍𝐀𝐓𝐈𝐎𝐍 :-
• Patient is drowsy, non responsive
• Pallor is present
• No cyanosis , clubbing , icterus, lymphadenopathy, pedal edema
𝐕𝐢𝐭𝐚𝐥𝐬 :-
• BP :- 130/90 mmHg
• PR :- 109bpm
• Temperature :- 102°F
• Grbs :- 86 mg/dl
𝐒𝐘𝐒𝐓𝐄𝐌𝐈𝐂 𝐄𝐗𝐀𝐌𝐈𝐍𝐀𝐓𝐈𝐎𝐍 :-
𝗖𝗩𝗦 :‐ S1 S2 heard, no murmurs
𝗥𝗦 :‐ Normal vesicular breath sounds hears
𝗣/𝗔 :- No tenderness, no palpable mass
𝗖𝗡𝗦 :-
1. 𝗛𝗜𝗚𝗛𝗘𝗥 𝗠𝗘𝗡𝗧𝗔𝗟 𝗙𝗨𝗡𝗖𝗧𝗜𝗢𝗡𝗦 :-
• Drowsy and non responsive
• MMSE couldn't be assessed
• Speech : nil
• Behavior : couldn't be assessed
• Memory : couldn't be assessed
• Intelligence : couldn't be assessed
• Lobar Functions : couldn't be assessed
𝗖𝗥𝗔𝗡𝗜𝗔𝗟 𝗡𝗘𝗥𝗩𝗘 𝗘𝗫𝗔𝗠𝗜𝗡𝗔𝗧𝗜𝗢𝗡 :-
• 3rd,4th,6th : pupillary reflexes present.
• No Nystagmus
𝗠𝗢𝗧𝗢𝗥 𝗘𝗫𝗔𝗠𝗜𝗡𝗔𝗧𝗜𝗢𝗡 :-
Right Left
UL LL UL LL
• Bulk N N N N
• Tone hyper hyper N N
• Power couldn't be assessed
𝗦𝗨𝗣𝗘𝗥𝗙𝗜𝗖𝗜𝗔𝗟 𝗥𝗘𝗙𝗟𝗘𝗫𝗘𝗦 :-
• Corneal : present present
• Conjunctival: present present
• Plantar : flexor mute
𝗗𝗘𝗘𝗣 𝗧𝗘𝗡𝗗𝗢𝗡 𝗥𝗘𝗙𝗟𝗘𝗫𝗘𝗦 :-
• Biceps 2+ 1+
• Triceps 2+ 1+
• Supinator 2+ 1+
• Knee 2+. 1+
• Ankle 2+. 1+
𝗦𝗘𝗡𝗦𝗢𝗥𝗬 𝗘𝗫𝗔𝗠𝗜𝗡𝗔𝗧𝗜𝗢𝗡 :-
• couldn't be assessed
𝐏𝐑𝐎𝐕𝐈𝐒𝐈𝐎𝐍𝐀𝐋 𝐃𝐈𝐀𝐆𝐍𝐎𝐒𝐈𝐒 :-
• Rt CVA with left hemiplegia with global aphasia
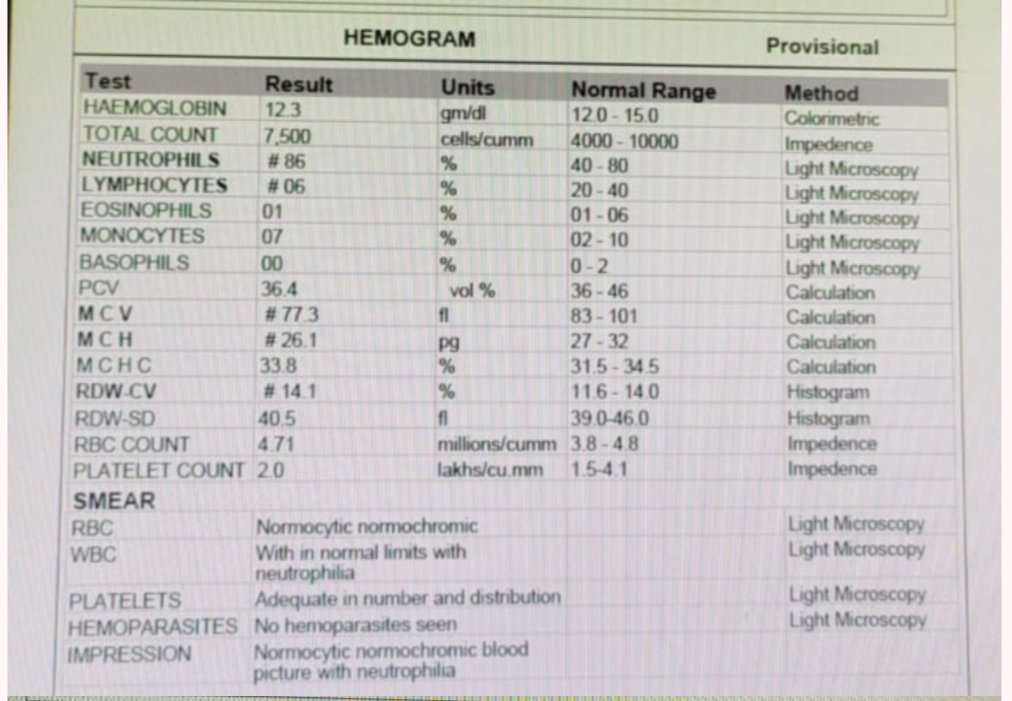
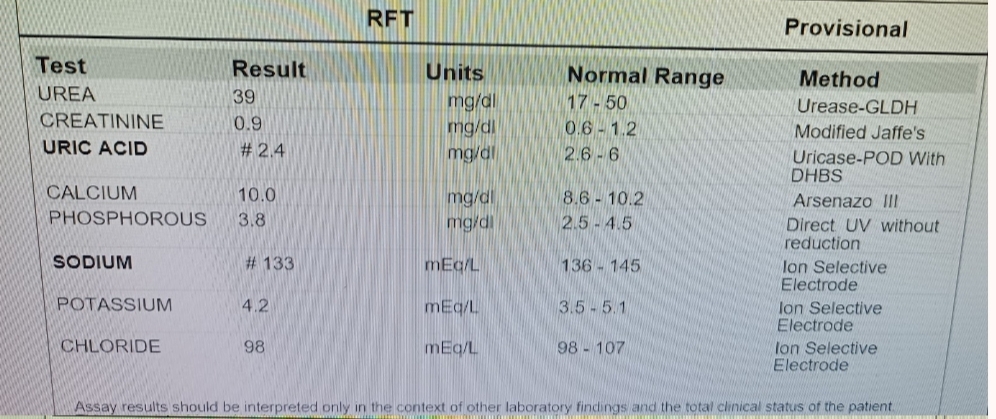
𝐈𝐍𝐕𝐄𝐒𝐓𝐈𝐆𝐀𝐓𝐈𝐎𝐍𝐒 :-


Chest xray

RBS - 86 mg/dl
Mri
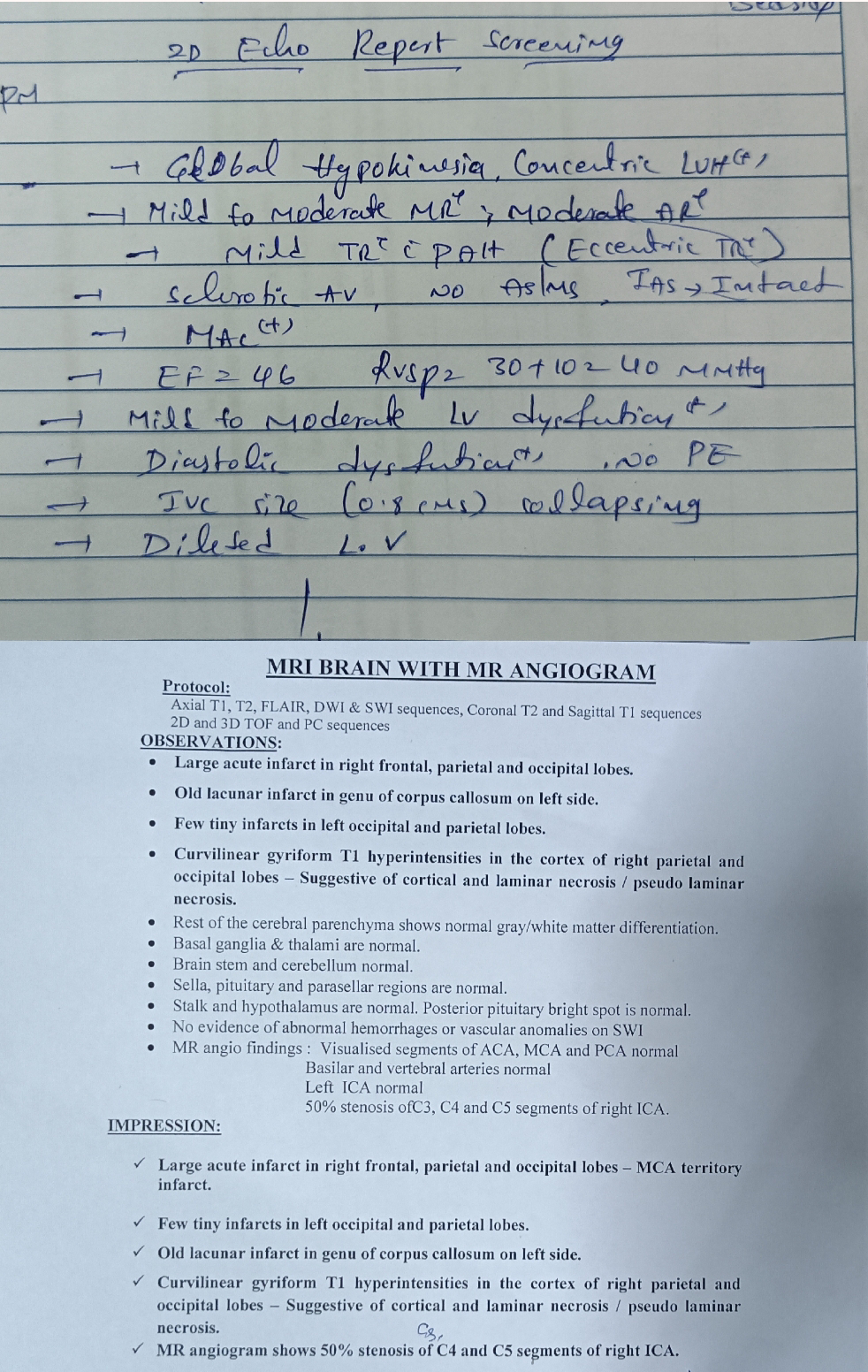
𝐃𝐈𝐀𝐆𝐍𝐎𝐒𝐈𝐒 :-
Right sided CerebroVascular Accident with left sided Hemiplegia with involvement of area supplied by middle cerebral artery due to embolism .
𝐏𝐋𝐀𝐍 𝐎𝐅 𝐌𝐀𝐍𝐀𝐆𝐄𝐌𝐄𝐍𝐓
1) Ryle 's tube
2) IV FLUIDS
3) Tab ECOSPRIN 150 MG RT STAT
F/B TAB ECOSPRIN 75 mg RT OD
4)Tab ROSUVASTATIN 40 MG RT STAT
F/B TAB ROSUVASTATIN 20 MG RT OD
5) TAB CLOPIDOGREL 150 Mg RT STAT
F/B TAB CLOPIDOGREL 75 mg RT OD